
That sharp pinch in the front of your groin when you twist? It’s not just a strain. For athletes, it’s often a hip labral tear, which is damage to the fibrocartilaginous rim that seals and protects the hip socket. You’re likely an athlete under 40, playing sports like soccer, basketball, or hockey, where repetitive hip rotation is the norm. You’ve probably been told it’s “just tightness,” but the pain persists. This guide cuts through the noise to explain exactly what’s happening inside your joint, how doctors actually see the damage, and whether surgery is your only path back to the field.
Quick Takeaways for Athletes
- Diagnosis isn’t guesswork: Standard MRIs miss up to 65% of tears. Magnetic Resonance Arthrography (MRA) is the gold standard for imaging with 90-95% accuracy.
- Surgery isn’t always first: Conservative care works for about two-thirds of athletes, but only if underlying structural issues like dysplasia aren’t ignored.
- Timing matters: Return to sport takes 3-4 months for debridement but 5-6 months for repair. Rushing this process increases re-tear risk significantly.
- Anatomy dictates outcome: If you have hip dysplasia, fixing the labrum alone has a 65% failure rate. The socket structure must be addressed too.
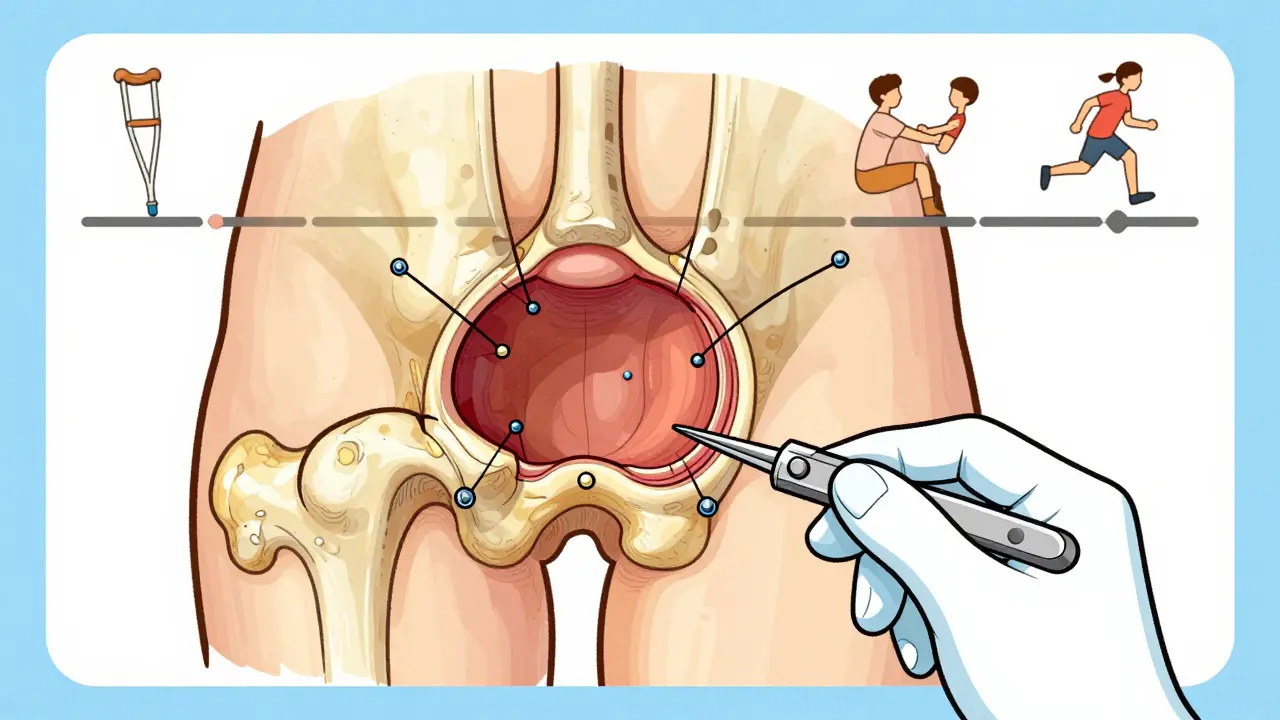
What Is a Hip Labral Tear?
Your hip joint is a ball-and-socket design. The acetabulum is the cup-shaped socket in your pelvis, and the femoral head is the ball. Lining the rim of that socket is the labrum-a ring of tough, rubbery cartilage. Think of it as a gasket on a car engine; it creates suction to keep the ball centered and absorbs shock during impact.
When that gasket tears, the seal breaks. The most common cause isn’t a single traumatic event like a fall, but rather Femoroacetabular Impingement (FAI), which is a condition where abnormal bone growth causes the ball and socket to rub together instead of gliding smoothly. Every time you pivot, squat, or kick, those bony bumps pinch the labrum. Over time, it frays and tears. According to data from Cleveland Clinic, FAI is the primary driver behind the majority of these injuries in active populations.
You might feel a deep ache in the groin, stiffness after sitting, or a mechanical click. About 78% of patients with confirmed tears report pain during specific physical exam maneuvers like the FADIR test (flexion, adduction, internal rotation). If you’re an athlete, ignoring this can lead to accelerated wear on the articular cartilage, paving the way for early-onset osteoarthritis.
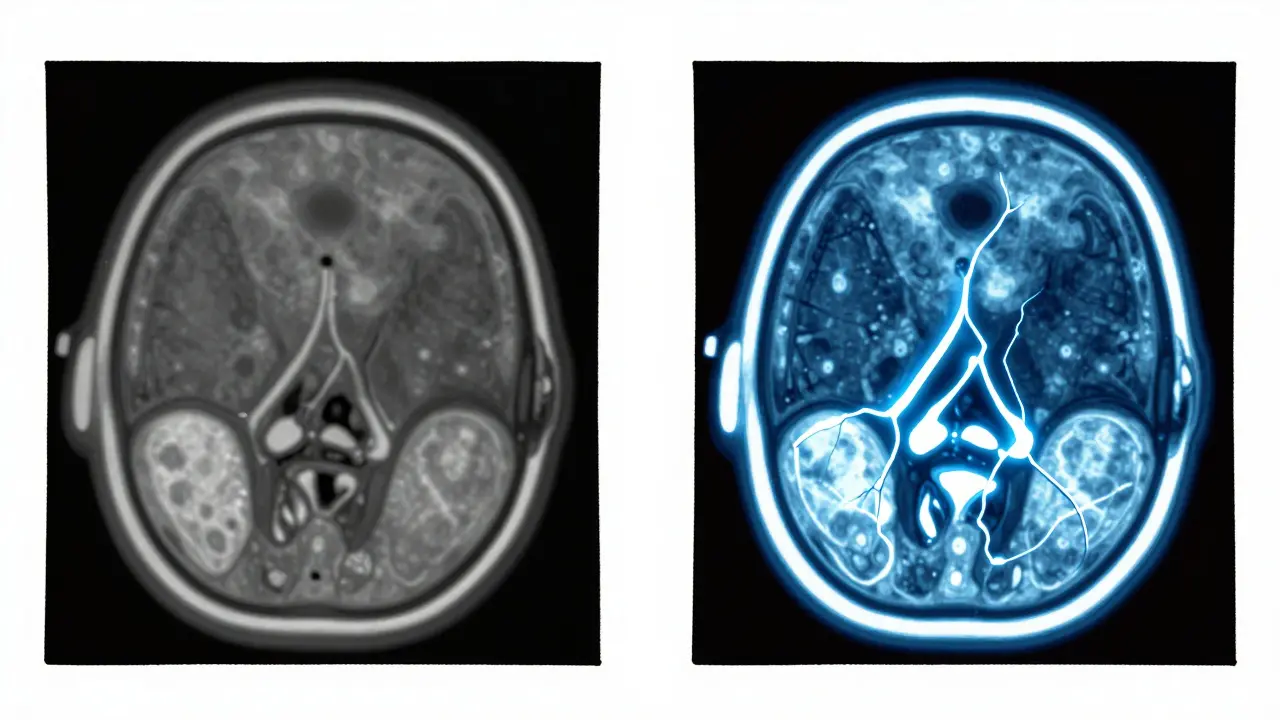
The Imaging Dilemma: Why Your MRI Might Be Wrong
Here’s the frustrating part: standard imaging often fails to catch the problem. A conventional MRI is a magnetic resonance imaging scan that uses strong magnets and radio waves to create detailed images of soft tissues has only 35-60% sensitivity for labral tears. That means more than half the time, a tear is present but invisible on the scan. Doctors might tell you everything looks fine, leaving you in limbo.
To get a clear picture, you need Magnetic Resonance Arthrography (MRA), which is an enhanced MRI procedure where contrast dye is injected directly into the hip joint before scanning. The dye fills the tiny gaps and cracks in the labrum, making them light up on the image. Studies show MRA boosts sensitivity to 90-95%. The International Hip Documentation Society recommends this as the preferred modality because standard MRI misses 30% of partial-thickness tears-tears that haven’t fully separated but are still causing significant pain and dysfunction.
Before any advanced imaging, doctors will start with plain X-rays. These don’t show the labrum itself, but they reveal the bone architecture. They look for signs of dysplasia (shallow socket) or cam/pincer lesions (bone spurs associated with FAI). This step is critical because treating the tear without addressing the bone shape is like patching a tire while driving over nails.
Conservative Care: Can You Avoid Surgery?
Not every tear requires an operating room. In fact, True Sports Physical Therapy reports that 65% of athletes manage their symptoms successfully without surgery. However, “conservative care” doesn’t mean doing nothing. It requires a structured approach.
- Relative Rest & Activity Modification: Stop the movements that pinch the joint. For runners, this might mean switching to cycling or swimming. For soccer players, avoiding sharp cuts and pivots is essential for 4-6 weeks.
- Anti-Inflammatories: NSAIDs like ibuprofen or naproxen help reduce synovitis (inflammation of the joint lining), which often accompanies the tear.
- Targeted Physical Therapy: This is the cornerstone. The goal isn’t just to stretch tight hips, but to strengthen the glutes and core to stabilize the femoral head. Poor stability forces the labrum to work overtime.
- Injections: Corticosteroid injections provide temporary relief in 70-80% of cases, lasting 3-6 months. Newer approaches using Platelet-Rich Plasma (PRP) show promise, with a 2022 trial at Hospital for Special Surgery finding 55% of patients avoided surgery at one year.
If you try this protocol for 3-6 months and still have pain, clicking, or giving way, conservative management has failed. Continuing to push through pain risks turning a manageable tear into a degenerative joint disease.
Hip Arthroscopy: The Surgical Solution
When non-surgical options run out, Hip Arthroscopy is a minimally invasive surgical procedure using small incisions and a camera to visualize and repair structures inside the hip joint becomes the standard. It’s not open surgery; surgeons make tiny portals to insert instruments. There are two main goals during the procedure:
- Debridement: Trimming away the torn, unstable flap of labral tissue. This removes the source of catching but doesn’t restore the seal. Recovery is faster, typically 3-4 months.
- Repair: Using suture anchors to stitch the labrum back to the acetabular rim. This restores the suction seal and protects the joint long-term. Recovery takes 5-6 months but offers better preservation against arthritis.
The choice between debridement and repair depends on the quality of the remaining tissue and your age. Younger athletes usually get repairs to preserve joint health. Recent advancements include bioabsorbable anchors, like Smith & Nephew’s BioX, which dissolve over time, eliminating the need for future hardware removal. Two-year data shows 89% success rates with these newer systems.
Rehabilitation: The Road Back to Sport
Surgery is only half the battle. The rehabilitation protocol is rigorous and non-negotiable. Trying to return early is the fastest way to ruin the repair. A typical timeline spans six months:
- Weeks 1-6 (Protection): Weight-bearing is limited. You’ll use crutches initially. Focus is on reducing swelling and restoring basic range of motion without stressing the repair.
- Weeks 7-12 (Strengthening): Progressive loading begins. Glute medius and core strengthening become priorities to control femoral head position.
- Weeks 13-20 (Sport-Specific Training): Agility drills, cutting, and plyometrics are introduced gradually. The joint must handle dynamic loads safely.
- Weeks 21-26 (Return to Sport): Full contact or high-intensity training resumes only if specific criteria are met.
Critical benchmarks for clearance include achieving 90% quadriceps strength symmetry compared to the uninjured leg and demonstrating pain-free hip internal rotation to 30 degrees. Without meeting these metrics, the risk of re-injury skyrockets.
Special Considerations for High-Demand Athletes
If you play hockey, ballet, or gymnastics, your situation is more complex. These sports require extreme ranges of motion. Data from HSS Sports Medicine Institute indicates a 25% higher complication rate for these athletes post-surgery. The demands placed on the repaired labrum are immense.
Furthermore, anatomical abnormalities play a huge role. If you have Hip Dysplasia, which is a congenital condition where the hip socket is too shallow to adequately cover the femoral head, isolated labral repair fails in 65% of cases within two years. Dr. Andrea Stracciolini from Boston Children’s Hospital notes that fixing the dysplasia surgically alongside the labral tear is often necessary. Ignoring the shallow socket leaves the labrum exposed to excessive shear forces, guaranteeing another tear.
| Factor | Conservative Care | Arthroscopic Repair |
|---|---|---|
| Success Rate | 65% symptom resolution | 85-90% return to pre-injury level |
| Time to Return | Variable (weeks to months) | 5-6 months average |
| Risk of OA Progression | Higher if untreated >10 years | Reduced with successful repair |
| Ideal Candidate | Mild tears, no structural FAI | Young athletes, mechanical symptoms |
Frequently Asked Questions
How do I know if my hip pain is a labral tear or just muscle strain?
Muscle strains usually improve with rest and stretching within a few weeks. Labral tears often persist despite rest and may involve mechanical symptoms like clicking, catching, or locking in the joint. Pain located deep in the groin rather than the side or buttock is also a key indicator of intra-articular pathology like a labral tear.
Why did my doctor order an MRA instead of a regular MRI?
Standard MRIs lack the sensitivity to detect many labral tears, missing up to 65% of cases. An MRA involves injecting contrast dye into the hip joint, which highlights even small fissures in the labrum, providing a much clearer diagnosis with 90-95% accuracy.
Can I return to competitive sports after hip arthroscopy?
Yes, most young athletes return to their pre-injury level of sport. Success rates are 85-90% for those under 40. However, sports requiring extreme hip flexion or rotation, like hockey or ballet, carry a slightly higher risk of complications and require a more cautious rehabilitation timeline.
What happens if I ignore a hip labral tear?
Ignoring a tear can lead to progressive damage to the articular cartilage of the hip joint. Untreated labral tears are associated with a 4.5 times higher risk of developing osteoarthritis within 10 years. Early intervention helps preserve joint function and delays or prevents arthritis.
Does insurance cover hip arthroscopy and MRA?
Coverage varies by provider and plan. While standard MRIs are widely covered, some insurers require prior authorization for MRAs, considering them specialized tests. Patients often face out-of-pocket costs ranging from $1,200 to $1,800 for MRAs if not fully covered. Always verify benefits with your insurer before scheduling advanced imaging.
Rachel Harrypersad
June 3, 2026 AT 17:46so you're telling me the standard mri is basically a lie detector that fails half the time. this is why people stay broken for years. doctors just look at the scan say its fine and send you home with ice packs while your cartilage disintegrates. it's not tightness. it's structural failure masked by incompetence. i hated my ortho for two years because he kept saying 'it's in your head' when every pivot felt like glass shards in my groin. stop trusting the default imaging protocol
Brian Irwin
June 5, 2026 AT 15:45i know exactly how frustrating that feels man. i went through the same thing with my soccer team back in college. we all thought it was just muscle strain because we stretched daily but nothing helped until someone suggested an mra. once they saw the tear everything changed. don't give up on finding answers because the first test said you were okay. your pain is real and there are specialists who actually know what to look for
Rosy Centire
June 7, 2026 AT 10:05The distinction between debridement and repair is absolutely critical here and often glossed over by general practitioners. Debridement is merely trimming the damage; it does not restore the suction seal of the labrum which is vital for long-term joint preservation. If you are under forty and have a reparable tear opting for debridement alone is essentially choosing early osteoarthritis. You must address the underlying FAI bone morphology or the repair will fail regardless of surgical skill. This is not a matter of opinion it is biomechanical fact.
Aswin Ashokan
June 8, 2026 AT 15:23in india we fix these issues without such expensive machines usually. physiotherapy works if you do it right. western medicine is too focused on surgery and money. most athletes recover with simple exercises and rest. this guide makes it sound complicated to scare people into paying more. lazy diagnosis leads to unnecessary operations. trust your body not the scanner
William Storm
June 9, 2026 AT 16:54One might ponder the sheer audacity of suggesting that a sixty-five percent failure rate for isolated repairs in dysplastic hips is merely a 'statistic.' It is, rather, a catastrophic oversight of anatomical reality. The article correctly identifies that patching the tire while driving over nails is futile, yet one wonders how many surgeons continue this practice out of convenience or financial incentive. The bioabsorbable anchors are a nice touch, I suppose, but they do little to mitigate the fundamental error of ignoring acetabular depth. Truly, the modern medical complex prefers the quick fix over the holistic correction.
Wendy Engelmann
June 10, 2026 AT 17:23it is interesting how the timeline shifts depending on the procedure. five months for repair versus three for debridement seems significant but the outcome difference is huge. i always thought rehab was just about getting strong again but realizing it is about restoring stability to control the femoral head changes everything. glute medius strength is probably the most underrated factor in hip health. people ignore their glutes until something breaks
Lisa Thomas
June 11, 2026 AT 06:50oh my god this is so scary!! i had that clicking sound for years and just ignored it thinking it was normal for dancers. now reading about the 65% failure rate if you have dysplasia makes me want to cry :(. i hope i dont need surgery but if i do i am definitely asking for the mra first. no more guessing games. thank you for sharing this information it really opened my eyes to what could be happening inside my joints :(
Nicholas Bowling
June 11, 2026 AT 18:48everyone says surgery is bad but sometimes it is the only way. i had mine done and now i can play hockey again. before that i was in constant pain and couldn't even walk properly. people complain about the recovery time but living in pain is worse. six months is nothing compared to a lifetime of arthritis. stop whining about the rehab and just get it fixed if conservative care fails. life goes on
Jay Foreman
June 13, 2026 AT 02:56look i respect the effort put into this guide but let's be real. insurance companies are the real enemy here. they deny mras and force you to try physical therapy for six months while your labrum tears further apart. i fought my insurer for three months to get the contrast dye injection approved. meanwhile my joint was deteriorating. the system is designed to keep you sick and poor. great info though but useless if you cant afford the diagnostic step